A hernia is one of those conditions that often starts as something you can easily ignore — a small, soft bulge that appears when you cough or strain and disappears when you lie down. It does not always hurt, at least not in the beginning. Life goes on, and the hernia quietly waits.But here is the critical thing about hernias — they do not get better on their own. They do not shrink. They do not disappear. Left untreated, they almost always grow larger over time, become more symptomatic, and carry the risk of a serious, life-threatening complication called strangulation, where the trapped tissue loses its blood supply and begins to die.Hernia is one of the most common surgical conditions in the world. In India, inguinal (groin) hernias alone are estimated to affect over 10 million people, with a significant proportion remaining untreated due to lack of awareness, fear of surgery, or financial considerations.The good news is that modern laparoscopic hernia repair is a safe, effective, and minimally invasive procedure with a very short recovery time — and in the hands of an experienced laparoscopic surgeon, it offers excellent long-term outcomes.In this comprehensive guide, Dr. Hamikchandra Patel — Fellowship-trained gastroenterologist and advanced laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad — explains hernias in complete detail: what they are, why they happen, how to recognise them, and why timely surgical treatment is the only definitive solution.
What is a Hernia?
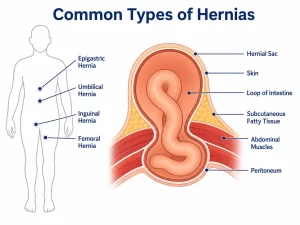
A hernia occurs when an internal organ or fatty tissue squeezes through a weak spot or gap in the surrounding muscle or connective tissue wall that normally holds it in place.Think of it like a tear in a tyre inner tube — when the inner rubber weakens, the air inside pushes through the gap and creates a visible bulge on the surface. A hernia works in a very similar way. The organ or tissue pushes through the weakened muscular wall and creates a lump or bulge under the skin, typically visible and often felt when you stand, cough, or strain.The abdomen is the most common site for hernias because the abdominal wall must balance the significant outward pressure exerted by the organs inside the abdomen against the structural integrity of its muscles and connective tissue. Any area of weakness — whether congenital, from a previous surgical incision, or developed over time through strain or ageing — becomes a potential hernia site.
Types of Hernia — A Complete Overview
Understanding the type of hernia is essential because different types present differently, occur in different populations, and may require different surgical approaches.Inguinal Hernia (Groin Hernia): By far the most common type of hernia, accounting for approximately 75 percent of all hernia cases. An inguinal hernia occurs when a part of the intestine or fatty tissue pushes through the inguinal canal — a passage in the groin area through which the spermatic cord passes in men and the round ligament passes in women.Inguinal hernias are far more common in men than women, largely due to anatomical differences. Men are approximately 10 times more likely to develop an inguinal hernia. They present as a bulge in the groin that may extend into the scrotum in men, and often cause a dragging discomfort or ache particularly after prolonged standing or physical activity.Femoral Hernia: Less common than inguinal hernias but more common in women, particularly older women. A femoral hernia occurs just below the inguinal ligament, where the femoral canal passes from the abdomen into the thigh. Femoral hernias are smaller but carry a higher risk of strangulation than inguinal hernias and should be repaired promptly after diagnosis.Umbilical Hernia: Occurs when tissue pushes through the abdominal wall near the navel (belly button). Umbilical hernias are extremely common in newborns — most close on their own by the age of two. In adults, they typically develop due to increased intra-abdominal pressure from obesity, multiple pregnancies, chronic cough, or ascites (fluid in the abdomen). Adult umbilical hernias do not resolve on their own and require surgical repair.Incisional Hernia: Develops through the scar of a previous abdominal surgical incision. When an abdominal wound heals, the resulting scar tissue is structurally weaker than the original muscle wall — making it susceptible to hernia formation, particularly when intra-abdominal pressure is elevated. Incisional hernias can develop months or even years after the original surgery. They can range from small and asymptomatic to very large and complex.Hiatus Hernia: A hiatus hernia is unique in that it occurs internally — inside the chest cavity rather than through the abdominal wall skin. It occurs when part of the stomach pushes upward through the diaphragm into the chest cavity through an opening called the hiatus. Hiatus hernias are a major contributing factor to GERD (acid reflux) and are extremely common in adults above 50 and in those who are obese. Small hiatus hernias are often managed medically. Large or symptomatic ones may require surgical repair.Epigastric Hernia: Occurs through a weakness in the midline of the abdomen between the navel and the breastbone. Usually contains fat rather than intestinal tissue. Often small and may cause localised tenderness or a visible lump.Spigelian Hernia: A relatively rare type that occurs along the outer edge of the rectus abdominis muscle — the muscle running vertically down the centre of the abdomen. Spigelian hernias can be difficult to diagnose clinically as they are often hidden beneath the surface without a visible external bulge and may require imaging for confirmation.
What Causes a Hernia?
A hernia develops from a combination of two factors: a weakness or defect in the muscle or connective tissue wall, and increased pressure within the abdomen that pushes tissue through that weakness.Congenital weakness: Some people are born with a naturally weaker abdominal wall at certain points. This is the most common underlying cause of inguinal hernias in men — a residual weakness from fetal development that never fully closed.Ageing: Muscles and connective tissue naturally lose strength and elasticity with age, making hernias more likely in middle-aged and older adults.Chronic straining during bowel movements: Constipation and the repeated effort of straining to pass stools is a significant risk factor — particularly for inguinal and umbilical hernias.Heavy lifting: Lifting heavy weights — particularly with poor technique — generates sudden, intense spikes in intra-abdominal pressure that can trigger hernia formation at a pre-existing weak point.Chronic cough: Conditions that cause persistent coughing — including asthma, chronic bronchitis, and smoking-related lung disease — repeatedly increase abdominal pressure and are a well-recognised hernia risk factor.Obesity: Excess body weight places constant, elevated pressure on the abdominal wall, weakening it progressively over time.Previous abdominal surgery: As explained above, surgical scars are structurally weaker than original tissue and are susceptible to incisional hernia development.Pregnancy: Multiple pregnancies stretch and weaken the abdominal wall muscles significantly, increasing the risk of umbilical and other ventral hernias.Ascites: Abnormal accumulation of fluid in the abdominal cavity, often associated with liver disease, creates massively elevated intra-abdominal pressure and commonly leads to umbilical hernia development.
Symptoms of a Hernia — What to Look and Feel For
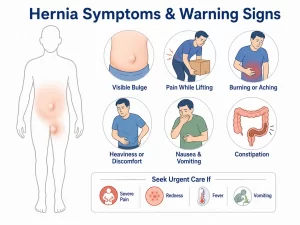
The symptoms of a hernia vary depending on its type, location, and size — but the most consistent finding across all types is a visible or palpable bulge.Visible bulge or lump: The most obvious and defining sign of most hernias. The bulge typically appears when you stand up, cough, sneeze, or strain — and may partially or fully disappear when you lie down. Over time, as the hernia enlarges, the bulge may become permanently visible even at rest.Aching, dragging, or heavy sensation: A dull ache, heaviness, or dragging discomfort in the area of the hernia — particularly after prolonged standing, walking, or physical activity. This sensation is caused by the weight of the herniated tissue pulling against the surrounding muscle wall.Sharp pain during exertion: Pain or discomfort when bending over, coughing, lifting, or straining. In early-stage hernias, this may be the only symptom.Scrotal swelling in men: In inguinal hernias that extend into the scrotum, there may be noticeable swelling and dragging pain in one side of the scrotum. This can sometimes be mistaken for a scrotal condition.Symptoms of obstruction: When the intestine is trapped in the hernia and partially blocked, symptoms include nausea, vomiting, abdominal distension, inability to pass gas or stools, and cramping abdominal pain. This is a warning sign requiring urgent medical evaluation.Symptoms of strangulation — a medical emergency: Strangulation occurs when the herniated tissue becomes so tightly trapped that its blood supply is completely cut off. Symptoms include sudden, severe pain at the hernia site, a bulge that becomes hard, red, and tender, fever, nausea, and vomiting. Strangulated hernias are surgical emergencies — if not treated within hours, the affected tissue begins to die and the situation becomes life-threatening. Any hernia patient experiencing sudden severe pain should go to an emergency department immediately.
Diagnosing a Hernia
In most cases, a hernia is diagnosed clinically — through a physical examination by an experienced surgeon who can feel and observe the bulge. The patient is often asked to stand up and cough, which makes the hernia more prominent and easier to assess.Ultrasound: Useful for confirming small or uncertain hernias and for assessing the contents of the hernia sac.CT scan: The most detailed imaging tool for complex hernias — particularly incisional hernias, recurrent hernias, or when multiple defects are suspected. A CT scan provides the surgeon with a precise map of the hernia anatomy before planning the repair.MRI: Used in selected cases where soft tissue detail is particularly important for surgical planning.
Treatment — Why Surgery is the Only Definitive Solution
This is a point worth stating clearly: there is no medication, no exercise programme, no truss or belt, and no dietary change that can repair a hernia. The only definitive treatment for a hernia is surgery.Trusses and support belts can manage symptoms temporarily in patients who are unfit for surgery, but they do not treat the hernia and carry the risk of masking the symptoms of a developing strangulation.The goal of hernia surgery is to return the herniated tissue to its proper position and repair the weakness in the abdominal wall — either with sutures alone or, more commonly in modern practice, by reinforcing the repair with a surgical mesh that significantly reduces the risk of recurrence.Open hernia repair: The traditional approach, performed through a single larger incision over the hernia site. Still widely used and highly effective for many hernia types. Recovery typically takes 3 to 6 weeks for full return to normal activity.
Laparoscopic hernia repair — the modern gold standard:
Laparoscopic hernia repair has transformed hernia surgery over the past two decades. Rather than a single large incision, three small incisions (typically less than 1 cm each) are made in the abdomen. A tiny camera and specialised surgical instruments are inserted, and the hernia is repaired from inside — returning the herniated tissue to its correct position and placing a surgical mesh over the defect from within to reinforce the repair.The advantages of laparoscopic hernia repair over open surgery are substantial:Significantly less post-operative pain — the internal approach avoids large muscle incisions.Much faster recovery — most patients return to light activity within 3 to 5 days and to full normal activity including light work within 1 to 2 weeks.Shorter hospital stay — typically 24 hours or less.Lower risk of wound complications and infection.Better visualisation — the camera provides a magnified, high-definition view of the hernia and surrounding structures, allowing more precise repair.Particularly advantageous for bilateral inguinal hernias (hernias on both sides of the groin) — both can be repaired simultaneously through the same three small incisions.Lower recurrence rates when performed by an experienced laparoscopic surgeon.Dr. Hamikchandra Patel performs advanced laparoscopic hernia repair — including TEP (Totally Extraperitoneal) and TAPP (Transabdominal Preperitoneal) techniques for inguinal and femoral hernias, and laparoscopic ventral hernia repair for umbilical and incisional hernias — at Shaleen Multi Speciality Hospital, Sola, Ahmedabad.
Who Should Have Their Hernia Repaired — and When?
The general principle is that all symptomatic hernias should be repaired, and sooner is better than later.A hernia that is causing pain, discomfort, or activity limitation should be repaired without significant delay. Waiting allows the hernia to enlarge, makes repair more complex, and increases the risk of serious complications.For truly asymptomatic hernias — particularly small inguinal hernias in men — some surgeons recommend watchful waiting with regular monitoring. However, studies show that the majority of asymptomatic inguinal hernias become symptomatic within five years, and emergency repair of a strangulated hernia carries significantly higher risks than elective repair. Most experienced surgeons therefore recommend elective repair for all confirmed hernias in patients who are medically fit for surgery.Femoral hernias and incisional hernias carry higher strangulation risks and should be repaired promptly regardless of symptoms.
Conclusion
A hernia is not an emergency you need to panic about — but it is a condition that demands attention and action. Ignoring a hernia does not make it go away. It makes it larger, more symptomatic, and increasingly risky. The window between a straightforward elective repair and a dangerous emergency operation is something no patient should gamble with.Modern laparoscopic hernia surgery has made hernia repair safer, faster, and far less disruptive to daily life than it has ever been before. With the right surgeon and the right technique, most patients are back to normal within a week.Dr. Hamikchandra Patel is a Fellowship-trained laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad, with extensive experience in advanced laparoscopic hernia repair for all hernia types. If you have noticed a bulge, experienced groin or abdominal discomfort, or have been told you have a hernia and are unsure about your next step — a consultation is all it takes to get clarity.To book your appointment with Dr. Hamikchandra Patel, visit drgastro.in or contact Shaleen Multi Speciality Hospital, Sola, Ahmedabad today.
After a heavy meal, a burning sensation rises in your chest. You reach for an antacid, it settles down, and you forget about it. The next evening, it happens again. A week later, the same. Before long, the antacid packet is a permanent fixture on your bedside table, your office desk, and in your bag.Sound familiar? If it does, you are far from alone.Acidity is arguably the most universal digestive complaint in India. Survey after survey consistently shows that a significant proportion of the Indian adult population experiences acidity symptoms at least once a week — and millions experience it daily. The combination of spicy food, irregular mealtimes, high stress, and sedentary lifestyles makes acidity almost an occupational hazard of modern Indian life.But here is what most people do not know — occasional acidity and chronic acid reflux are two very different things. One is a common, manageable inconvenience. The other is a medical condition called Gastroesophageal Reflux Disease, or GERD, that can cause serious long-term damage to your oesophagus if left untreated.In this comprehensive guide, Dr. Hamikchandra Patel — gastroenterologist and laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad — explains everything you need to understand about acidity and acid reflux: what causes it, how to recognise when it has crossed a line, and what your treatment options are.
Understanding Acidity — What is Actually Happening in Your Body?
To understand acidity, you first need to understand how your stomach works.Your stomach produces hydrochloric acid — a powerful digestive fluid that breaks down the food you eat and kills harmful bacteria. The stomach lining is specially designed to withstand this acid. However, the oesophagus — the food pipe that connects your mouth to your stomach — is not protected in the same way.Between the oesophagus and the stomach sits a muscular valve called the lower oesophageal sphincter (LOS). Under normal circumstances, this valve opens to allow food to pass into the stomach and then closes tightly to prevent stomach acid from flowing back upward.Acidity occurs when this valve weakens, relaxes inappropriately, or malfunctions — allowing stomach acid to escape upward into the oesophagus. The acid then irritates the sensitive lining of the oesophagus, producing the familiar burning sensation in the chest or throat that we call heartburn or acidity.When this happens occasionally after a heavy meal or a particularly spicy dish, it is normal and not a cause for concern. When it happens consistently — two or more times per week over a period of weeks — it qualifies as Gastroesophageal Reflux Disease (GERD), a chronic condition that requires proper medical evaluation and treatment.
What is the Difference Between Acidity, Acid Reflux, Heartburn, and GERD?
These four terms are often used interchangeably, but they are not quite the same thing:Acidity: A broad, colloquial term used in India to describe the general sensation of excess acid in the stomach or chest. It covers everything from mild post-meal discomfort to chronic reflux symptoms.Acid reflux: The specific physical process of stomach acid flowing backward into the oesophagus. It is the mechanism behind the symptom.Heartburn: The burning sensation in the chest or throat that results from acid reflux. It is a symptom, not a disease. The name is misleading — it has nothing to do with the heart.GERD (Gastroesophageal Reflux Disease): A diagnosed chronic medical condition characterised by persistent, frequent acid reflux that occurs more than twice a week and causes ongoing symptoms and potentially damage to the oesophageal lining. GERD requires medical treatment beyond lifestyle changes alone.
What Causes Acidity and Acid Reflux?
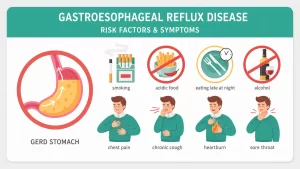
Acidity can be triggered or worsened by a wide range of factors — dietary, lifestyle-related, physiological, and medication-related. Understanding your personal triggers is an important part of managing the condition.Dietary triggers: Spicy food, oily and fried food, citrus fruits, tomatoes, onions, garlic, chocolate, carbonated beverages, tea, and coffee are among the most common dietary triggers for acid reflux. These foods either increase acid production, relax the lower oesophageal sphincter, or both.Eating habits: Eating large meals, eating too quickly, lying down immediately after eating, or skipping meals and then overeating in one sitting all increase the risk of acid reflux.Excess body weight: Obesity is one of the strongest risk factors for GERD. Excess abdominal fat puts physical pressure on the stomach, pushing acid upward into the oesophagus more easily.Smoking: Nicotine directly weakens the lower oesophageal sphincter and increases stomach acid production. Smokers have significantly higher rates of GERD than non-smokers.Alcohol: Alcohol relaxes the lower oesophageal sphincter, stimulates stomach acid secretion, and directly irritates the oesophageal lining — a triple trigger for acid reflux.Hiatus hernia: A condition where part of the stomach pushes up through the diaphragm into the chest cavity. Hiatus hernia significantly weakens the lower oesophageal sphincter and is one of the most common structural causes of chronic GERD.Medications: Certain commonly used medications can worsen acid reflux, including aspirin and other NSAIDs (like ibuprofen), certain blood pressure medications, antidepressants, and osteoporosis drugs. If you are on long-term medication and experiencing frequent acidity, discuss this with your doctor.Pregnancy: Hormonal changes during pregnancy relax the lower oesophageal sphincter, and the growing uterus puts upward pressure on the stomach — making heartburn and acid reflux extremely common in the second and third trimesters.Stress and anxiety: While stress does not directly cause acid reflux, it heightens the perception of pain and discomfort and can trigger or worsen symptoms through indirect physiological mechanisms including changes in gut motility and acid secretion.
Symptoms of Acidity and GERD
The symptoms of acidity and acid reflux range from the very familiar to some that are not immediately associated with the digestive system:Heartburn: The classic symptom — a burning sensation in the centre of the chest, typically starting behind the breastbone and sometimes rising toward the throat. It often worsens after eating, when lying down, or when bending forward.Regurgitation: A sour or bitter-tasting fluid rising into the back of the throat or mouth. Sometimes described as a wet burp. In severe cases, partially digested food comes back up.Bloating and belching: Excess gas, a feeling of fullness, and frequent burping — particularly after meals.Nausea: Particularly in the mornings or after eating, especially when GERD is associated with delayed stomach emptying.Dysphagia (difficulty swallowing): A sensation of food getting stuck in the throat or chest while swallowing. This symptom, when present, should always be evaluated promptly as it can indicate oesophageal narrowing from long-standing GERD.Chronic cough: A persistent dry cough, particularly at night, that does not respond to standard cough treatment. Many people do not realise that acid reflux can irritate the airways and trigger a chronic cough without any prominent heartburn.Hoarseness or sore throat: Acid reaching the throat and voice box can cause persistent hoarseness, a feeling of a lump in the throat (globus sensation), and chronic throat clearing — often misdiagnosed as a throat infection.Worsening asthma: In patients with pre-existing asthma, GERD can trigger or significantly worsen asthmatic symptoms. If your asthma seems poorly controlled despite medication, GERD may be a contributing factor worth investigating.
When Does Acidity Stop Being Normal?
This is perhaps the most important question in this entire article — and the one that most people do not have a clear answer to.Occasional acidity is normal. A heavy dinner, a celebration with rich food, a particularly stressful week — these are all situations where temporary acidity is expected and does not indicate any underlying condition.However, you should consult a gastroenterologist without delay if:You experience heartburn or acid reflux symptoms two or more times per week consistently.Your symptoms are not adequately controlled by over-the-counter antacids.You are taking antacids daily or several times a week for more than two weeks.You experience difficulty or pain while swallowing.You notice unintentional weight loss alongside your acidity symptoms.You experience persistent nausea or vomiting.You notice black or tarry stools, or blood in your vomit — these indicate bleeding in the digestive tract and require immediate emergency attention.You are above 40 years of age and experiencing new, persistent acidity symptoms for the first time.You have a long history of GERD and have not had a recent endoscopy to monitor your oesophageal health.Persistent, untreated GERD causes real damage to the oesophagus over time and carries the risk of serious complications including oesophagitis, Barrett's oesophagus, and oesophageal strictures.
Complications of Untreated Chronic Acid Reflux
This is the section that transforms casual acidity sufferers into patients who take their condition seriously:Oesophagitis: Chronic acid exposure inflames and erodes the lining of the oesophagus, causing ulcers, bleeding, and pain. Left untreated, it worsens progressively.Oesophageal stricture: Repeated damage and healing of the oesophageal lining causes scar tissue to build up, narrowing the oesophagus over time. This leads to increasing difficulty swallowing and requires endoscopic dilation to treat.Barrett's oesophagus: A potentially serious condition in which the normal lining of the lower oesophagus is replaced by abnormal cells — a direct response to long-term acid damage. Barrett's oesophagus is a recognised precursor to oesophageal cancer and requires regular endoscopic surveillance.Oesophageal cancer (adenocarcinoma): Long-standing, untreated GERD — particularly when it progresses to Barrett's oesophagus — carries an increased risk of oesophageal cancer. This is one of the most serious reasons why persistent GERD should never be left unmonitored.These complications are not inevitable — but they are real, and they are preventable with timely diagnosis and appropriate treatment.
How is GERD Diagnosed?
Clinical evaluation: In most cases, a detailed history of your symptoms is sufficient for an initial diagnosis of GERD. Your doctor will ask about the frequency, duration, and character of your symptoms, your dietary and lifestyle habits, and your medication history.Upper GI Endoscopy (OGD Scopy): The most important diagnostic tool for GERD evaluation. A thin, flexible camera is passed through the mouth into the oesophagus, stomach, and duodenum, allowing direct visualisation of any inflammation, ulcers, strictures, or Barrett's changes. Dr. Hamikchandra Patel performs upper GI endoscopy at Shaleen Multi Speciality Hospital, Sola, Ahmedabad.pH monitoring: A small probe placed in the oesophagus measures the actual amount of acid exposure over a 24-hour period. This is particularly useful when symptoms are atypical or when endoscopy results are inconclusive.Barium swallow study: An X-ray-based test where you swallow a barium contrast solution, making the oesophagus and stomach visible on X-ray. Useful for identifying hiatus hernia and oesophageal strictures.Oesophageal manometry: Measures the pressure and function of the lower oesophageal sphincter and oesophageal muscles. Used when surgical treatment is being considered.
Treatment Options for Acidity and GERD
Lifestyle modifications — the foundation of treatment:No medical treatment for GERD works optimally without accompanying lifestyle changes. These are not optional extras — they are a core part of effective GERD management.Eat smaller, more frequent meals rather than two or three large meals. Avoid lying down for at least two to three hours after eating. Elevate the head of your bed by 15 to 20 cm if you experience nighttime reflux symptoms. Lose excess weight if applicable — even a 5 to 10 percent reduction in body weight significantly reduces GERD symptoms. Quit smoking. Limit alcohol. Identify and avoid your personal dietary triggers.Antacids: Provide rapid but short-lived symptom relief by neutralising stomach acid already present. Suitable for occasional, mild symptoms only. Not a long-term solution for chronic GERD.H2 blockers: Medications like famotidine reduce the amount of acid the stomach produces. More effective than antacids for moderate symptoms and provide longer-lasting relief.Proton pump inhibitors (PPIs): The most effective medication class for GERD. Drugs like omeprazole, pantoprazole, and rabeprazole suppress acid production at its source. PPIs are highly effective for healing oesophagitis and controlling GERD symptoms. They are typically prescribed for 4 to 8 week courses, with dosage and duration guided by your doctor. Long-term PPI use should always be monitored by a gastroenterologist.
For patients with confirmed GERD who do not respond adequately to medication, who experience significant side effects from long-term PPIs, or who have a large hiatus hernia contributing to their reflux, surgery is a highly effective and durable treatment option.Laparoscopic Nissen fundoplication is the gold standard surgical procedure for GERD. The upper portion of the stomach is wrapped around the lower end of the oesophagus, reinforcing the weakened lower oesophageal sphincter and preventing acid from refluxing upward. The procedure is performed laparoscopically — through small incisions — with a short hospital stay and quick recovery. Most patients experience complete or near-complete relief from reflux symptoms long-term.
Conclusion
Acidity may be one of the most common complaints in India, but that does not make it trivial. Chronic, untreated acid reflux causes progressive damage to the oesophagus and carries real risks — including the development of Barrett's oesophagus and oesophageal cancer — that no amount of antacid can prevent.If you have been managing your acidity with daily antacids for weeks or months, or if your symptoms are frequent, severe, or accompanied by any of the warning signs described in this article, please do not delay seeking a specialist consultation.Dr. Hamikchandra Patel is a Fellowship-trained gastroenterologist at Shaleen Multi Speciality Hospital, Sola, Ahmedabad, with extensive experience in the diagnosis and management of GERD, oesophageal conditions, and the full spectrum of upper GI disorders. To book your consultation, visit drgastro.in or contact us today.
Piles is one of those medical conditions that a large number of people silently suffer from for years without seeking help. The discomfort is real, the impact on daily life is significant, but the topic carries enough social stigma in India that most patients delay consulting a doctor — sometimes for years — hoping the problem will resolve on its own.It rarely does. And in the meantime, what starts as mild discomfort can progress into a painful, bleeding, and severely uncomfortable condition that interferes with every aspect of daily life.The truth is that piles — medically known as haemorrhoids — is an extremely common condition. Research suggests that nearly 75 percent of people will experience haemorrhoids at some point in their lifetime, and in India, it is estimated that over 75 million people are currently affected. It is not a condition to be ashamed of, and more importantly, it is a condition that is very effectively treated.In this comprehensive guide, Dr. Hamikchandra Patel — gastroenterologist and laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad — explains piles in complete detail: what it is, why it develops, how to identify it, and what your treatment options are at every stage.
What Are Piles (Haemorrhoids)?
Haemorrhoids are swollen, inflamed veins located in and around the rectum and anus. They are similar in nature to varicose veins — the same process of vein swelling and engorgement that occurs in the legs can occur in the blood vessels of the lower rectum.Under normal circumstances, these veins exist in everyone — they are a natural part of the anal canal's vascular structure and play a role in controlling bowel movements. The problem arises when they become enlarged, inflamed, or prolapsed due to increased pressure over time.Piles is not a dangerous or life-threatening condition in most cases, but it can cause significant bleeding, pain, itching, and discomfort — and in advanced stages, it requires surgical intervention to resolve.
Types of Piles — Internal vs External
Understanding the type of piles you have is important because it determines the symptoms you experience and the treatment approach that is most appropriate.Internal haemorrhoids: Located inside the rectum, above the dentate line. Because there are very few pain-sensitive nerves in this area, internal haemorrhoids are often painless — but they bleed easily during bowel movements. In more advanced cases, they can prolapse — meaning they push out through the anal opening.External haemorrhoids: Located under the skin around the anus, below the dentate line. This area has many pain-sensitive nerves, which is why external haemorrhoids are often painful, particularly when they become thrombosed (when a blood clot forms inside the vein). They may appear as a lump or swelling around the anus.Mixed haemorrhoids: A combination of both internal and external haemorrhoids occurring together, which is quite common in advanced or long-standing cases.
The Four Grades of Internal Haemorrhoids
Internal haemorrhoids are classified into four grades based on their severity. This grading system directly guides treatment decisions.Grade I: The haemorrhoid is present inside the rectum but does not prolapse. The main symptom is bleeding during bowel movements — typically fresh, bright red blood on the toilet paper or in the toilet bowl. No lump or protrusion is felt.Grade II: The haemorrhoid prolapses out of the anus during straining or bowel movement but returns inside on its own without any manual assistance. Bleeding continues and mild discomfort may be felt.Grade III: The haemorrhoid prolapses during bowel movement and does not return inside on its own — it needs to be pushed back manually with a finger. At this stage, discomfort, mucus discharge, and itching become more pronounced alongside bleeding.Grade IV: The haemorrhoid is permanently prolapsed outside the anus and cannot be pushed back inside even manually. This grade involves significant pain, constant discomfort, heavy bleeding, and often requires surgical treatment.
What Causes Piles?
Piles develop when the veins around the lower rectum and anus are subjected to prolonged or excessive pressure that causes them to stretch and swell. The most common contributing factors include:Chronic constipation: Straining during bowel movements is one of the leading causes of haemorrhoids in India. The effort of passing hard, infrequent stools puts intense pressure on the rectal veins repeatedly over time.Low-fibre diet: A diet low in fruits, vegetables, and whole grains leads to harder stools and constipation — directly increasing haemorrhoid risk.Prolonged sitting on the toilet: Spending extended time on the toilet — a very common habit, often compounded by phone use — creates sustained pressure on the anal veins.A sedentary lifestyle: Lack of physical activity slows digestion, contributes to constipation, and reduces healthy blood circulation in the pelvic region.Pregnancy: The growing uterus puts increasing pressure on the pelvic veins during pregnancy. Combined with hormonal changes that relax vein walls, haemorrhoids are extremely common in pregnant women, particularly in the third trimester.Obesity: Excess body weight increases pressure on the pelvic and rectal veins chronically.Chronic diarrhoea: Repeated loose stools cause frequent straining and irritation of the anal area, which can also trigger haemorrhoid development.Ageing: The tissues supporting the veins in the rectum and anus naturally weaken with age, making haemorrhoids more likely in people above 45.Heredity: A family history of haemorrhoids increases your personal risk, suggesting a genetic predisposition to weaker vein walls in the rectal area.
Symptoms of Piles — Recognising the Warning Signs
Symptoms of piles vary depending on the type and grade. Here are the most common ones to be aware of:Rectal bleeding: The most common symptom of internal haemorrhoids. You may notice bright red blood on toilet paper after wiping, drops of blood in the toilet bowl, or blood on the surface of your stool. Importantly, this blood is always bright red — dark or tarry blood suggests bleeding higher in the digestive tract and requires separate investigation.Pain and discomfort around the anus: More characteristic of external haemorrhoids, particularly when thrombosed. The pain can range from mild soreness to sharp, severe pain that makes sitting and walking uncomfortable.Itching or irritation: A persistent itching sensation in and around the anus, often caused by mucus secretion from prolapsed haemorrhoids irritating the surrounding skin.A lump near the anus: A soft, fleshy lump that is tender to touch, located around the anus — indicative of an external haemorrhoid or a prolapsed internal haemorrhoid.Sensation of incomplete bowel emptying: Many patients with internal haemorrhoids feel as though their bowel has not emptied completely even after a bowel movement — a sensation caused by the bulk of the prolapsed tissue.Mucus discharge: A small amount of mucus or slime on the toilet paper or in underwear, often accompanied by mild itching and skin irritation around the anus.Faecal soiling: In advanced cases where haemorrhoids prevent complete anal closure, involuntary leakage of small amounts of faecal matter can occur.
When Should You See a Doctor?
Many people manage mild piles symptoms at home for a period of time with dietary changes and over-the-counter creams. However, you should consult a gastroenterologist without delay if:You notice any rectal bleeding — even if you suspect it is from piles, bleeding should always be evaluated by a doctor to rule out other causes including colorectal polyps or colorectal cancer.Your symptoms are not improving after two weeks of dietary changes and home management.You are experiencing significant pain that is interfering with daily activities.A prolapsed haemorrhoid cannot be pushed back inside.You are experiencing mucus discharge, skin irritation, or soiling.Dr. Hamikchandra Patel at Shaleen Multi Speciality Hospital, Sola, Ahmedabad, provides comprehensive evaluation and treatment for all grades of haemorrhoids, from early-stage conservative management to advanced surgical procedures.
Treatment Options for Piles
Treatment for piles depends on the grade and severity of the condition. There is a clear progression from conservative management to minimally invasive procedures to surgery as the grade advances.Dietary and lifestyle changes (all grades, first-line treatment):Increasing fibre intake through fruits, vegetables, whole grains, and legumes is the single most effective long-term measure for managing and preventing piles. High-fibre diets soften stools, reduce straining, and decrease pressure on rectal veins. Aim for 25 to 30 grams of fibre per day.Drinking 8 to 10 glasses of water daily prevents hard stools. Avoiding prolonged toilet sitting, taking short walks after meals, and establishing a regular bowel routine all contribute meaningfully to symptom relief.Topical medications: Over-the-counter haemorrhoid creams and suppositories containing hydrocortisone, lidocaine, or witch hazel can reduce inflammation, pain, and itching temporarily. These manage symptoms but do not treat the underlying haemorrhoid.Rubber band ligation (Grade I, II, and some Grade III): A very effective, quick, and largely painless office procedure for internal haemorrhoids. A small rubber band is placed at the base of the haemorrhoid, cutting off its blood supply. The haemorrhoid shrinks and falls off within 7 to 10 days. No anaesthesia is required and most patients resume normal activities the same day. Multiple sessions may be needed for multiple haemorrhoids.Sclerotherapy (Grade I and II): A chemical solution is injected into the haemorrhoid tissue, causing it to shrink and harden. Best suited for smaller internal haemorrhoids. Quick, minimally invasive, and performed as an outpatient procedure.Infrared coagulation (Grade I and II): A beam of infrared light is used to create scar tissue at the base of the haemorrhoid, cutting off its blood supply and causing it to shrink. Another effective office-based procedure for early-grade haemorrhoids.
Surgical treatment — when is it necessary?
Surgery becomes the recommended treatment when haemorrhoids are Grade III or Grade IV, when minimally invasive procedures have failed or are not suitable, when thrombosed external haemorrhoids are causing severe pain, or when significant bleeding is not controlled by other means.Conventional haemorrhoidectomy: Surgical removal of the haemorrhoid tissue under spinal or general anaesthesia. Highly effective with excellent long-term results. Recovery typically takes 2 to 3 weeks and may involve some post-operative pain.Stapled haemorrhoidopexy (PPH — Procedure for Prolapse and Haemorrhoids): A technique particularly suited for Grade III and IV prolapsed haemorrhoids. A circular stapling device is used to remove a ring of the prolapsed tissue and staple the remaining tissue back into its normal position inside the anal canal. The staple line is above the pain-sensitive dentate line, resulting in significantly less post-operative pain compared to conventional haemorrhoidectomy. Recovery is faster — most patients are discharged within 24 hours.Laser haemorrhoidoplasty: A newer technique using laser energy to shrink haemorrhoid tissue from within. It is minimally invasive, involves minimal bleeding, and offers faster recovery. Suitable for Grade I to Grade III haemorrhoids.Dr. Hamikchandra Patel is experienced in the full range of surgical and non-surgical haemorrhoid treatments and will recommend the most appropriate option based on your specific grade, symptoms, and overall health.
Can Piles Be Prevented?
While there is no absolute guarantee of prevention — particularly if you have a family history or have been pregnant — the following measures significantly reduce your risk and prevent recurrence after treatment:Eat a high-fibre diet consistently — this is the single most effective preventive measure.Stay well hydrated throughout the day — at least 8 glasses of water daily.Do not strain during bowel movements — if passing stool requires significant effort, your diet needs more fibre and water.Never ignore the urge to have a bowel movement — delaying increases the chance of constipation.Limit time spent sitting on the toilet — avoid reading or using your phone during bowel movements.Exercise regularly — even a 30-minute daily walk improves bowel regularity and pelvic circulation.Maintain a healthy body weight — obesity is a significant and modifiable risk factor for haemorrhoids.
Conclusion
Piles is far more common than most people realise — and far more treatable than most people fear. The key is to stop suffering in silence and seek medical attention before a manageable Grade I or Grade II condition progresses into a Grade III or Grade IV problem that requires surgery.With modern minimally invasive techniques and advanced surgical options available today, treating piles is straightforward, effective, and associated with very good long-term outcomes.If you are experiencing any of the symptoms described in this article — bleeding, pain, itching, lumps, or prolapse — do not delay your consultation.Dr. Hamikchandra Patel is a Fellowship-trained gastroenterologist and laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad, with extensive experience in the diagnosis and treatment of haemorrhoids at every grade. To book your consultation, visit drgastro.in or call us today.
You have just come back from an ultrasound and the report says the three words nobody wants to read — gallbladder stones detected. Your mind immediately fills with questions. How serious is this? Will I need surgery? Can it be treated with medication? What happens if I ignore it?If this sounds familiar, you are not alone. Gallbladder stones — medically known as cholelithiasis — are one of the most commonly diagnosed digestive conditions in India. Studies suggest that anywhere between 4 to 7 percent of the Indian adult population has gallbladder stones, with the numbers significantly higher among women, people above 40, and those with a family history of the condition.The good news is that gallbladder stones are well understood, manageable, and in most cases, completely treatable with modern laparoscopic surgery that requires just one to two days of hospitalisation.In this comprehensive guide, Dr. Hamikchandra Patel — Fellowship-trained gastroenterologist and laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad — explains everything you need to know about gallbladder stones: what they are, why they form, how to recognise them, and when surgery becomes necessary.
What is the Gallbladder?
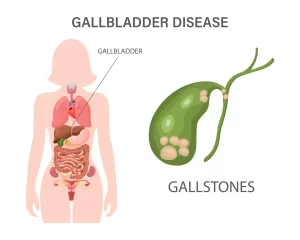
Before understanding gallbladder stones, it helps to understand the organ itself.The gallbladder is a small, pear-shaped organ located just beneath the liver, on the upper right side of your abdomen. Its primary job is to store bile — a digestive fluid produced by the liver that helps break down fats in the food you eat.When you eat a fatty meal, the gallbladder contracts and releases bile into the small intestine through a duct called the common bile duct. When you are not eating, bile is stored and concentrated in the gallbladder.The gallbladder is not a vital organ — which means the human body can function perfectly normally without it. This is an important fact to understand early, because it explains why surgical removal of the gallbladder (cholecystectomy) is a safe and permanent solution for gallbladder stones without long-term consequences for your health.
What Exactly Are Gallbladder Stones?
Gallbladder stones are hardened deposits that form inside the gallbladder when the substances that make up bile — primarily cholesterol, bile salts, and bilirubin — become imbalanced and crystallise over time.They can range in size from a tiny grain of sand to a golf-ball-sized lump. Some people develop a single large stone. Others develop hundreds of small stones simultaneously. Both situations can cause significant problems.There are two main types of gallbladder stones:Cholesterol stones: The most common type in India, accounting for approximately 80 percent of all gallbladder stone cases. These yellow-green stones form when bile contains too much cholesterol and not enough bile salts to dissolve it.Pigment stones: Smaller, darker stones that form when bile contains excess bilirubin. These are more commonly associated with liver conditions like cirrhosis, biliary tract infections, or certain blood disorders.
What Causes Gallbladder Stones?
Gallbladder stones do not form overnight — they develop gradually over months or years when the chemical composition of bile is disrupted. The key contributing factors include:Excess cholesterol in bile: When the liver produces more cholesterol than bile can dissolve, the excess crystallises and forms stones. This is the most common cause.Excess bilirubin: Certain medical conditions — including liver cirrhosis, biliary tract infections, and blood disorders like sickle cell anaemia — cause the liver to produce too much bilirubin, which can lead to pigment stone formation.Incomplete emptying of the gallbladder: If the gallbladder does not empty completely or often enough, bile becomes overly concentrated, creating conditions favourable for stone formation.Dietary habits: A diet consistently high in fatty, oily, or cholesterol-rich foods and low in fibre increases the risk significantly.Prolonged fasting or skipping meals: When you skip meals regularly, the gallbladder is not stimulated to release bile frequently enough, leading to bile concentration and stagnation.Rapid weight loss: Crash dieting or very rapid weight loss causes the liver to release extra cholesterol into bile, increasing stone formation risk.
Who is at Higher Risk of Gallbladder Stones?
While gallbladder stones can develop in anyone, certain factors significantly increase the risk. These are often remembered using the classic medical mnemonic — the 5 Fs:Female: Women are approximately twice as likely as men to develop gallbladder stones, particularly during or after pregnancy and in women who take estrogen-based hormonal medication.Fat: Being overweight or obese increases the amount of cholesterol the liver secretes into bile.Forty: The risk of gallbladder stones increases progressively after the age of 40.Fertile: Pregnancy increases bile cholesterol levels and reduces gallbladder motility, making pregnant and recently pregnant women a higher-risk group.Family history: A family history of gallbladder stones significantly increases your personal risk, indicating a genetic component in bile composition.Additional risk factors include diabetes, rapid weight loss, a sedentary lifestyle, and a diet consistently high in refined carbohydrates and saturated fats.
Gallbladder Stone Symptoms — How Do You Know You Have Them?
This is where gallbladder stones become complicated — because many people have them without ever knowing it.Silent gallstones: Approximately 60 to 80 percent of people with gallbladder stones experience no symptoms at all. These are called silent gallstones and are often discovered incidentally during an ultrasound done for a completely different reason. Silent stones do not always require immediate treatment but do require monitoring.When gallbladder stones do cause symptoms, the most common and distinctive one is biliary colic — a sudden, intense pain in the upper right side of the abdomen that often radiates to the right shoulder or back. This pain typically occurs after eating a heavy or fatty meal and can last anywhere from 30 minutes to several hours before subsiding.Other symptoms to watch for include:Pain in the upper right or centre of the abdomen: Often described as a squeezing, cramping, or stabbing pain. It may come and go or remain constant.Nausea and vomiting: Frequently accompany gallstone attacks, particularly after fatty meals.Indigestion, bloating, and gas: Chronic indigestion that does not respond to antacids can sometimes be linked to gallbladder stones.Jaundice: A yellowing of the skin and eyes that indicates a stone has migrated into the common bile duct and is blocking bile flow. This is a serious symptom requiring immediate medical attention.Dark urine and pale stools: These accompany jaundice and indicate bile duct obstruction.Fever and chills: When a gallstone causes infection in the gallbladder (cholecystitis) or bile duct, fever develops. This is a medical emergency.
Complications of Untreated Gallbladder Stones
Many patients, particularly those with mild or intermittent symptoms, delay treatment hoping the problem will resolve on its own. This is a risky decision. Untreated gallbladder stones that begin causing symptoms can lead to serious, potentially life-threatening complications:Acute cholecystitis: Inflammation of the gallbladder caused by a stone blocking the cystic duct. Symptoms include severe, persistent pain, fever, and tenderness in the abdomen. Requires urgent hospitalisation.Choledocholithiasis: When a stone migrates from the gallbladder into the common bile duct, it can block the flow of bile from the liver to the small intestine. This causes jaundice, severe pain, and requires urgent intervention.Cholangitis: A serious bacterial infection of the bile duct, usually resulting from bile duct obstruction by a stone. This is a medical emergency with a significant mortality risk if not treated promptly.Acute pancreatitis: Gallstones are one of the leading causes of acute pancreatitis in India. When a stone temporarily blocks the pancreatic duct outlet, it triggers severe inflammation of the pancreas, causing intense abdominal pain, vomiting, and potentially organ damage.Gallbladder perforation: In severe, prolonged cases of untreated cholecystitis, the gallbladder wall can rupture, spilling bile into the abdominal cavity and causing a life-threatening infection called peritonitis.The presence of symptoms — even mild, occasional ones — is a signal that your gallbladder stones are active and that medical evaluation is necessary without delay.
How Are Gallbladder Stones Diagnosed?
Ultrasound: The most commonly used and most reliable diagnostic tool for gallbladder stones. An abdominal ultrasound detects stones with an accuracy of over 95 percent and is completely non-invasive and painless.Blood tests: A complete blood count (CBC), liver function tests (LFT), and serum amylase/lipase tests help assess whether stones have caused infection, bile duct obstruction, or pancreatitis.CT scan: Provides a more detailed view of the gallbladder and surrounding structures, particularly useful when complications are suspected.MRCP (Magnetic Resonance Cholangiopancreatography): A specialised MRI-based imaging technique used to visualise the bile ducts in detail — particularly when a stone in the common bile duct is suspected.ERCP (Endoscopic Retrograde Cholangiopancreatography): Both a diagnostic and therapeutic procedure. When stones are found in the common bile duct, ERCP allows the doctor to remove them endoscopically without surgery.
Treatment Options for Gallbladder Stones
Watchful waiting (for silent gallstones): If gallbladder stones are discovered incidentally and are causing absolutely no symptoms, your doctor may recommend monitoring them with periodic ultrasounds rather than immediate surgery. However, this approach is only suitable for confirmed asymptomatic cases.Medications: Certain oral medications like ursodeoxycholic acid can slowly dissolve small cholesterol stones over a period of months to years. However, this approach is rarely used in practice because the success rate is low, treatment duration is long, and stones frequently recur after medication is stopped.ERCP for bile duct stones: When stones have migrated into the common bile duct, ERCP is used to locate and remove them endoscopically. This is often done before gallbladder surgery when both duct stones and gallbladder stones are present simultaneously.Laparoscopic cholecystectomy — the gold standard treatment: For symptomatic gallbladder stones, surgical removal of the gallbladder is the most effective and permanent solution. Laparoscopic cholecystectomy involves making three to four small incisions (typically less than 1 cm each) in the abdomen, inserting a small camera and surgical instruments, and removing the gallbladder completely.The procedure is performed under general anaesthesia and typically takes 30 to 60 minutes. Most patients are discharged within 24 hours and return to normal daily activities within one week. The recovery is far faster and less painful than traditional open surgery.Dr. Hamikchandra Patel performs laparoscopic cholecystectomy at Shaleen Multi Speciality Hospital, Sola, Ahmedabad, using advanced laparoscopic equipment and following internationally established surgical protocols.
Life After Gallbladder Removal — What to Expect
Patients frequently worry about what life looks like without a gallbladder. The reassuring reality is that most people experience no significant long-term dietary restrictions or digestive problems after the gallbladder is removed.In the immediate weeks after surgery, the liver continues producing bile as before — but without the gallbladder as a reservoir, bile now flows directly and continuously into the small intestine rather than being stored and released in concentrated bursts. This continuous flow is sufficient for normal digestion in most people.Some patients experience mild, temporary loose stools or diarrhoea in the weeks following surgery as the body adjusts to the new bile flow pattern. This typically resolves on its own within four to six weeks.Most patients return to a completely normal diet within four to six weeks of surgery, with no permanent restrictions.
Conclusion
Gallbladder stones are common, well-understood, and highly treatable. The key is not to ignore symptoms and not to wait until a complication develops before seeking medical advice.If you have been diagnosed with gallbladder stones, or if you are experiencing recurring pain in the upper right abdomen, nausea after fatty meals, or unexplained indigestion, a specialist consultation is the right next step.Dr. Hamikchandra Patel is a Fellowship-trained gastroenterologist and advanced laparoscopic surgeon at Shaleen Multi Speciality Hospital, Sola, Ahmedabad. With extensive experience in laparoscopic cholecystectomy and the full spectrum of digestive and hepatobiliary conditions, Dr. Patel provides comprehensive, personalised care for gallbladder stone patients.To book a consultation, call us or visit drgastro.in today.