Fatty Liver Disease in Ahmedabad: Causes, Warning Signs & When You Must See a Gastroenterologist
Introduction
Fatty liver disease has quietly become one of the most prevalent health conditions in Ahmedabad — and most people who have it do not know. It shows no symptoms in its early stages. It does not cause pain. It is not detected by a blood test alone. It is discovered, more often than not, as an incidental finding on an ultrasound done for an entirely different reason — and by that time, it may already have been present and progressing for years. This is the silent epidemic that is affecting an estimated 1 in 3 urban Indian adults in 2026. Driven by sedentary lifestyles, calorie-dense diets, rising rates of diabetes and obesity, and increasing metabolic syndrome in Ahmedabad's working population — Non-Alcoholic Fatty Liver Disease (NAFLD) is now the leading cause of chronic liver disease in India. This guide covers what fatty liver disease is, the stages of progression, the warning signs that should never be ignored, and how Dr. Hamik Chandra Patel at Shaleen Hospital, Sola, Ahmedabad diagnoses and treats it.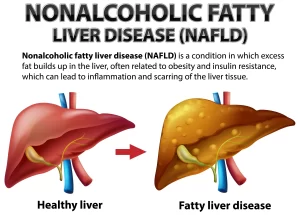
What Is Fatty Liver Disease?
Fatty liver disease occurs when excess fat accumulates in the liver cells. The liver normally contains a small amount of fat — but when fat comprises more than 5–10% of the liver's total weight, it is classified as a fatty liver. There are two main types:NAFLD — Non-Alcoholic Fatty Liver Disease
Fat accumulation in the liver in people who drink little or no alcohol. NAFLD is the most common liver condition in India, directly linked to metabolic factors: obesity, diabetes, high cholesterol, high triglycerides, and insulin resistance.AFLD — Alcoholic Fatty Liver Disease
Fat accumulation caused by regular heavy alcohol consumption. The liver's capacity to metabolise alcohol is exceeded, and fat accumulates. In Ahmedabad, NAFLD is by far the more prevalent — affecting middle-class, non-drinking, vegetarian adults who consume a diet high in refined carbohydrates, sugar, and fried foods.The 4 Stages of NAFLD — Understanding Progression
NAFLD is not a single condition — it is a spectrum that progresses through four stages if not addressed:Stage 1: Simple Fatty Liver (Steatosis)
Fat accumulates in liver cells but there is no inflammation or damage. Completely reversible with lifestyle changes. No symptoms. Often found incidentally on ultrasound.Stage 2: NASH (Non-Alcoholic Steatohepatitis)
Fat accumulation with active inflammation and early liver cell damage. This is the dangerous transition point — NASH can progress to fibrosis and cirrhosis. May still be asymptomatic or present with mild fatigue.Stage 3: Fibrosis
Repeated inflammation causes scar tissue (fibrosis) to form in the liver. Liver function starts to decline. Some reversibility remains with aggressive treatment.Stage 4: Cirrhosis
Extensive scarring replaces normal liver tissue. Liver function is significantly compromised. Largely irreversible — risk of liver failure and liver cancer. Symptoms become apparent and serious. The critical insight: Most patients are diagnosed at Stage 1 or 2 — when the condition is completely manageable and reversible. This is exactly why recognising risk factors and getting evaluated is so important.Who Is at Risk? Fatty Liver Risk Factors in Ahmedabad
| Risk Factor | How It Contributes |
| Obesity (BMI > 25–30) | Most powerful risk factor — excess fat overloads liver metabolism |
| Type 2 Diabetes | Insulin resistance drives fat deposition in liver cells |
| High triglycerides | Elevated blood fats directly increase liver fat storage |
| High LDL cholesterol | Metabolic dysregulation associated with NAFLD |
| Metabolic syndrome | The combination of obesity, diabetes, hypertension, and dyslipidaemia |
| Sedentary lifestyle | Reduces fat metabolism and increases insulin resistance |
| High-sugar, high-carb diet | Refined flour, sugar, and sweetened beverages are converted to liver fat |
| Rapid weight loss | Paradoxically, crash dieting or bariatric complications can worsen NAFLD |
| PCOD / hormonal disorders | Women with PCOD have elevated NAFLD risk |
| Hypothyroidism | Thyroid dysfunction associated with metabolic NAFLD |
| Age 40–60 | Risk increases with age as metabolic rate declines |
Warning Signs of Fatty Liver Disease — When Your Liver Is Struggling
The frustrating reality of NAFLD is that early stages produce no symptoms. But as the condition progresses — particularly to NASH, fibrosis, or cirrhosis — symptoms begin to emerge:Early-to-Intermediate Symptoms (Stage 2–3)
- Fatigue — persistent, unexplained tiredness not explained by other causes
- Upper right abdominal discomfort — a dull ache or heaviness under the right rib cage (where the liver sits)
- Mild nausea — particularly after fatty meals
- Reduced appetite — feeling full quickly
Advanced Symptoms (Stage 3–4: Fibrosis/Cirrhosis)
- Jaundice — yellowing of skin and whites of eyes (serious sign)
- Abdominal swelling (ascites) — fluid accumulation in the abdomen
- Leg swelling (oedema)
- Easy bruising or bleeding — liver's clotting function failing
- Itching — bile salt accumulation in the skin
- Confusion or difficulty concentrating (hepatic encephalopathy) — toxins not cleared by the compromised liver
- Dark urine and pale stools
Why May 2026 Is World Digestive Health Month — Act Now
May is globally recognised as World Digestive Health Month — an annual initiative by the World Gastroenterology Organisation to raise awareness about preventable digestive diseases. NAFLD is one of the headline conditions for 2026 — reflecting the global recognition of its epidemic scale. For Ahmedabad residents who have been told their ultrasound shows a "mildly echogenic liver" or "fatty changes" — or who have risk factors but have never been evaluated — May is the ideal time to book a specialist consultation.Diagnosis of Fatty Liver Disease at Dr. Gastro's Clinic, Ahmedabad
1. Blood Tests
- Liver function tests (LFTs): ALT and AST elevation suggests liver inflammation (NASH)
- Lipid profile: Triglycerides and cholesterol assessment
- Fasting glucose and HbA1c: Diabetes and insulin resistance screening
- CBC and coagulation studies: Assessing liver function in advanced disease
- Note: Normal LFTs do not rule out NAFLD — many patients with fatty liver have completely normal blood tests
2. Ultrasound Abdomen
First-line, non-invasive test. Identifies fat accumulation as "increased echogenicity" of the liver. Can also detect advanced fibrosis signs and complications like ascites. Cannot reliably distinguish steatosis from NASH.3. FibroScan (Transient Elastography)
A non-invasive, painless test that measures liver stiffness — indicating the degree of fibrosis. Far more informative than ultrasound for staging NAFLD. Dr. Hamik uses FibroScan at Shaleen Hospital to stage liver disease without the need for biopsy in most cases.4. Liver Biopsy
The gold standard for definitive NAFLD staging. A small tissue sample is taken from the liver under ultrasound guidance and examined under microscope. Reserved for cases where non-invasive tests are inconclusive or where staging will significantly alter management.5. MRI / CT Scan
Used in selected cases for detailed liver assessment and to rule out complications.
Treatment of Fatty Liver Disease at Dr. Gastro's Clinic
The Single Most Important Treatment: Weight Loss
For overweight patients with NAFLD, a 5–10% reduction in body weight consistently reduces liver fat, decreases inflammation (NASH), and can reverse early fibrosis. This is the most evidence-based intervention available for NAFLD. Dr. Hamik works with patients on a structured, medically supervised weight management programme — combining dietary modification, physical activity, and metabolic optimisation.Dietary Modifications Specific to Ahmedabad Patients
- Eliminate or drastically reduce: refined flour (maida), white rice, sugar, sweetened beverages, fried snacks (farsan, chakli, sev), and ultra-processed foods
- Increase: vegetables, fruits, whole grains, legumes, nuts, and healthy fats (olive oil, nuts)
- Follow a Mediterranean-style diet — the most evidence-backed dietary pattern for NAFLD reduction
- Avoid: fruit juices, packaged foods labelled "low fat" (often high sugar), and alcohol
Exercise
Regular physical activity — both aerobic exercise (150 minutes/week) and resistance training — reduces liver fat independently of weight loss. Even modest increases in daily activity significantly improve NAFLD.Managing Associated Conditions
- Diabetes control: HbA1c optimisation reduces liver fat
- Lipid management: Statins, fibrates as appropriate
- Blood pressure control
- Thyroid optimisation
Medications
While there is currently no FDA-approved medication specifically for NAFLD, Dr. Hamik uses evidence-based pharmacological approaches including:- Vitamin E — for non-diabetic NASH patients
- Pioglitazone — for NASH with diabetes/prediabetes
- GLP-1 analogues (semaglutide, liraglutide) — showing strong benefit in NAFLD/NASH with obesity
- New NASH-specific agents currently in Phase 3 trials