Understanding and Treating Anal Canal Disorders in Ahmedabad: Symptoms, Diagnosis, and Treatment
Introduction
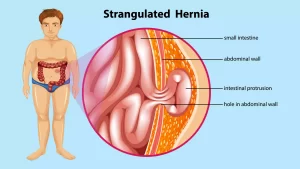
Conditions affecting the anal canal are among the most common health problems in India — yet they are among the most commonly left untreated. Whether it is the discomfort of piles (haemorrhoids) that has been managed with creams for months, a persistent itch that never goes away, a lump that appeared near the anus, or bleeding during bowel movements that has been dismissed as "nothing serious" — anal canal disorders affect millions of Indians and significantly reduce quality of life when left unaddressed. The hesitation to seek help is understandable. These conditions affect a private, sensitive part of the body, and many patients feel embarrassed discussing symptoms even with a doctor. But this delay costs them — conditions that are simple to treat in early stages can become complex, painful, and require more intensive surgery if left too long. This complete guide to anal canal disorders in Ahmedabad covers every common condition — piles, rectal prolapse, anal abscess, proctitis, perianal warts, and more — along with their symptoms, how they are diagnosed, and the full range of treatment options available at Dr. Gastro's clinic at Shaleen Multi Speciality Hospital, Sola, Ahmedabad.The Anatomy of the Anal Canal
Understanding what can go wrong begins with understanding the area's anatomy. The anal canal is the last 3–4 cm of the large intestine, ending at the anal opening (anus). It is surrounded by two rings of muscle — the internal anal sphincter (involuntary, always contracted) and the external anal sphincter (voluntary, under conscious control). Together, these muscles maintain continence — the ability to control bowel movements. The dentate line (also called the pectinate line) divides the anal canal into two zones:- Above the dentate line: No pain sensation (internal zone)
- Below the dentate line: Richly supplied with pain fibres (external zone — highly sensitive)
Common Anal Canal Disorders: Types, Symptoms, and Causes
1. Haemorrhoids (Piles) — Most Common
Piles — medically known as haemorrhoids — are the most frequently treated anal canal condition at Dr Gastro's clinic in Ahmedabad. They are swollen, enlarged blood vessels (vascular cushions) in and around the anal canal and rectum. Everyone has these vascular cushions — they are a normal part of anal anatomy that help with continence. Haemorrhoids develop when these cushions become engorged, prolapsed, or symptomatic.Types of Haemorrhoids
Internal Haemorrhoids: Develop above the dentate line (no pain fibres). Often asymptomatic initially, the first sign is usually bright red rectal bleeding on toilet paper or in the toilet bowl after a bowel movement. As they progress, they may prolapse (protrude outside the anal opening). Grading of Internal Haemorrhoids:| Grade | Description | Treatment |
| Grade I | Bulge into the anal canal, no prolapse | Diet, medication |
| Grade II | Prolapse during straining reduces spontaneously | Banding, medication |
| Grade III | Prolapse requires manual reduction | Banding, DGHAL, surgery |
| Grade IV | Permanently prolapsed, irreducible | Surgery required |
Causes and Risk Factors for Piles
- Chronic constipation or straining during bowel movements
- Low-fibre, high-spice diet — particularly common in Indian dietary patterns
- Prolonged sitting — especially during bowel movements
- Pregnancy (increased pelvic pressure)
- Obesity
- Chronic diarrhoea
- Family history
- Sedentary lifestyle
Symptoms of Piles
- Bright red bleeding from the anus during or after bowel movements
- A lump or swelling near the anal opening
- Itching, soreness, and irritation around the anus
- Pain and discomfort — especially with external haemorrhoids
- Mucous discharge after bowel movements
- Feeling of incomplete bowel emptying
2. Rectal Prolapse
Rectal prolapse occurs when the rectum (the lower portion of the large intestine) slides down from its normal position and protrudes through the anal opening. It is different from prolapsed haemorrhoids — in rectal prolapse, the full thickness of the rectal wall protrudes, typically appearing as concentric circular rings of pink/red tissue protruding from the anus. Rectal prolapse is more common in older women but can also occur in young children (usually resolving on its own) and is associated with chronic straining and weakened pelvic floor muscles.Types of Rectal Prolapse
- Mucosal prolapse: Only the inner lining of the rectum protrudes — often confused with large haemorrhoids
- Full-thickness prolapse: The entire thickness of the rectal wall protrudes — the more serious form
- Internal prolapse (intussusception): The rectum slides into itself internally without external protrusion
Symptoms
- Tissue or a mass protruding from the anus — initially only during straining, later permanently present
- Bright red rectal bleeding and mucus discharge
- Faecal incontinence — inability to fully control bowel movements
- Feeling of incomplete evacuation after bowel movements
- Anal discomfort, pain, and heaviness
3. Anorectal Abscess
An anorectal abscess is a collection of pus in the tissues around the anus and rectum, most commonly caused by infection of the small glands just inside the anus (anal crypts). These glands can become blocked, leading to bacterial infection and the formation of an abscess. Anorectal abscess is a medical emergency — it requires urgent drainage. Up to 50% of anorectal abscesses lead to the development of an anal fistula (an abnormal tunnel) after treatment.Types
- Perianal abscess: Most common — a painful swelling at the edge of the anus
- Ischiorectal abscess: A larger, deeper collection in the fat-filled space beside the rectum
- Intersphincteric abscess: Between the two sphincter muscles — often subtle but very painful
- Supralevator abscess: High abscess above the pelvic floor — rare but most complex
Symptoms
- Severe, throbbing, constant pain near the anus — worsening with sitting and walking
- A swollen, red, warm, tender lump near the anal opening
- Fever, chills, and general malaise
- Difficulty sitting comfortably
- Purulent (pus) discharge if the abscess spontaneously ruptures
4. Anal Warts (Condylomata Acuminata)
Anal warts are caused by the Human Papillomavirus (HPV) — a sexually transmitted infection. They appear as small, flesh-coloured growths around and inside the anus and can range from tiny pinpoints to large, cauliflower-like masses.Symptoms
- Small, soft, flesh-coloured lumps or bumps around the anal area
- Itching, burning, or moisture in the anal region
- Occasionally bleeding during bowel movements
- Many patients are completely asymptomatic — warts may be discovered incidentally
5. Proctitis — Inflammation of the Rectum
Proctitis is inflammation of the lining of the rectum. It can result from a number of causes, including inflammatory bowel disease (ulcerative colitis or Crohn's disease), radiation therapy (radiation proctitis), sexually transmitted infections, or rectal injury.Symptoms
- Frequent urge to have a bowel movement even when the rectum is empty (tenesmus)
- Rectal bleeding — ranging from mild spotting to significant blood
- Passage of mucus or pus from the rectum
- Rectal pain or a feeling of fullness and pressure
- Diarrhoea or frequent, small bowel movements
- Cramping in the lower abdomen
6. Anal Stenosis (Anal Stricture)
Anal stenosis is the abnormal narrowing of the anal canal, which makes it painful or difficult to pass stool. It can result from scarring after previous anal surgery, chronic inflammatory conditions, or radiation.Symptoms
- Difficulty passing stool; very narrow, pencil-thin stools
- Pain during bowel movements
- Constipation that does not respond to dietary changes
- Sensation of incomplete evacuation
7. Anal Skin Tags
Anal skin tags are small, soft, benign growths of skin around the outside of the anus. They commonly develop as a result of resolved external haemorrhoids or anal fissures. While they are not medically dangerous, they can cause hygiene concerns, itching, and discomfort.
Why Rectal Bleeding Should Never Be Ignored
One of the most important messages from this guide: rectal bleeding should always be evaluated by a specialist — never dismissed without investigation. While the most common causes of bright red rectal bleeding are benign (piles, fissures), rectal bleeding can also be a symptom of:- Colorectal cancer
- Rectal cancer
- Inflammatory bowel disease
- Rectal polyps
Diagnosis: How Dr Gastro Evaluates Anal Canal Disorders
Dr Hamik Chandra Patel is a specialist proctologist (a surgeon who specialises in diseases of the anus and rectum) — one of the very few in Sola, Ahmedabad — with expertise in diagnosing and treating the full spectrum of anal canal disorders.Diagnostic Process
- Clinical History: Detailed discussion of your symptoms — nature and duration of bleeding, location and character of pain, any discharge, change in bowel habits, associated weight loss, and relevant medical and surgical history.
- Perianal Inspection The specialist carefully examines the perianal skin for external haemorrhoids, skin tags, warts, fissures, abscesses, or fistula openings.
- Digital Rectal Examination (DRE) A gloved, lubricated finger is gently inserted into the anal canal to assess sphincter tone, feel for internal masses or haemorrhoids, and detect any tenderness suggesting abscess or other pathology.
- Proctoscopy: A short, lighted hollow tube (proctoscope) is inserted into the anal canal to directly visualise the anal canal and lower rectum. Essential for grading internal haemorrhoids, identifying the internal opening of fistulas, and detecting polyps or mucosal abnormalities.
- Sigmoidoscopy / Colonoscopy Used when rectal bleeding requires more thorough investigation to rule out colorectal cancer, polyps, inflammatory bowel disease, or proctitis affecting the colon. A flexible camera is passed through the anus to examine the rectum and colon.
- MRI and Imaging (for Complex Cases)
- MRI fistulogram: For complex anal fistulas — maps the tract and its relationship to sphincter muscles
- Transanal ultrasound: Assesses sphincter integrity in cases of incontinence or rectal prolapse
- CT scan: Used for suspected deep abscess or malignancy
Treatment Options for Anal Canal Disorders in Ahmedabad
Piles (Haemorrhoids) Treatment
Conservative Treatment (Grade I and II Piles):- A high-fibre diet and adequate hydration to soften stools
- Avoid straining during bowel movements; do not sit on the toilet for extended periods
- Sitz baths — warm water soaks after bowel movements for comfort
- Topical creams containing local anaesthetics and anti-inflammatory agents
- Stool softeners and laxatives were needed
- Minimally invasive with very small wound
- Less post-operative pain than conventional surgery
- Day surgery — home the same day
- Faster return to normal activity
- Low recurrence rate
Rectal Prolapse Treatment
Conservative (for mild mucosal prolapse):- Dietary fibre to prevent straining
- Pelvic floor physiotherapy to strengthen supporting muscles
- Rectopexy (Abdominal approach — laparoscopic): The rectum is mobilised and fixed to the sacrum (tailbone) to prevent future prolapse. Can be performed with or without mesh. This is the preferred approach for younger, fit patients.
- Delorme's Procedure / Altemeier's Procedure (Perineal approach): Performed through the anus — preferred for elderly or high-risk patients who cannot tolerate abdominal surgery.
Anorectal Abscess Treatment
Urgent incision and drainage (I&D): The only effective treatment for anorectal abscess. The abscess is opened under anaesthesia, pus is drained, and the cavity is cleaned. Antibiotics alone are not sufficient — drainage is always required. Post-drainage, follow-up at Dr Gastro's clinic monitors for the development of an anal fistula, which may require further treatment.Anal Warts Treatment
- Chemical destruction: Trichloroacetic acid (TCA) or podophyllin applied topically to destroy wart tissue
- Electrocautery or laser ablation: For larger or more extensive warts
- Surgical excision: For very large or resistant warts
- Immunomodulatory therapy: Imiquimod cream to stimulate the immune response against HPV
Proctitis Treatment
Treatment depends on the underlying cause:- Infectious proctitis: Antibiotics or antiviral medication
- Inflammatory proctitis (IBD-related): Anti-inflammatory medication (mesalazine), corticosteroid enemas
- Radiation proctitis: Sucralfate enemas, argon plasma coagulation, or laser treatment